Chapter 115. Orthopedic and Musculoskeletal Problems: Image Library
Orthopedic problems are common in neonates. The problems can be isolated deformities or as part of a generalized disorder. Usually these deformities are obvious, but a comprehensive musculoskeletal examination is the key for diagnosis of associated generalized disorders. This image library is a companion to Chapter 115: Orthopedic and Musculoskeletal Problems and provides images of some of the common problems encountered in the neonatal intensive care unit. These images are designated by the symbol ☼ in the text of the 7th edition of Neonatology.
The Chapter was authored and the images provided by Drs. Ahmed Thabet and William McKenzie.
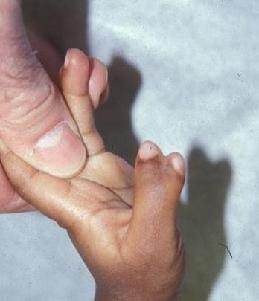
Polydactyly is duplication of one or more fingers. It is most common among African Americans. It may be associated with Ellis-van Creveld syndrome or chromosomal anomalies. Ulnar polydactyly, postaxial type may affect the little finger. It has autosomal dominant inheritance with variable penetration.
Thumb polydactyly, preaxial type. It affects the thumb.
Ulnar polydactly
Thumb polydactly
Syndactyly is a congenital webbing between the fingers. The fusion may be complete if it extends to the fingertips or complex if it involves the bony elements of the adjacent digits. It may be an isolated anomaly or associated with chromosomal or genetic disorders (eg, trisomy 21,13,18, Silver syndrome, Prader-Willi syndrome, or focal dermal hypoplasia). It is more common in boys, often with bilateral involvement. Also it is more common in the ring and middle finger than the index and thumb. Surgical reconstruction is often indicated in the first year of life to allow for development of hand function.
Syndactly
Torticollis is a lateral tilt of the neck and head typically due to a tight sternocleidomastoid muscle. The head and neck tilt toward the involved side and the chin is turned toward the contralateral side. Congenital muscular torticollisis due to fibrosis of the sternomastoid muscle, which may be due to a localized compartment syndrome or uterine packing problems.
Torticollis
Spina bifida is a group of disorders is characterized by congenital malformation of the spinal cord and vertebral column. Whereas the etiology of spina bifida is unknown, inadequate maternal intake of folic acid, gestational diabetes, and history of previously affected siblings with the same partner are contributory factors. The diagnosis can be made prenatally by elevated maternal serum α-fetoprotein, by ultrasound, or postnatally by the presence of the lesion in the neonate’s back. A tuft of hair over the neonate’s lumbosacral spine or skin dimple may be a sign of underlying anomalies.
Hair tuft in spina bifida
Developmental dysplasia of the hip (DDH)is a wide spectrum of hip abnormalities ranging from hip instability to frank dislocation. In certain cultures newborn cradling may be an etiologic factor in DDH (eg, using the cradleboard with the hip extended and adducted by American Indians). Hip examinations usually demonstrate hip instability. These tests are used for clinical screening of the neonates:
Ortolani test (reduction test for the dislocated hip). The child should be positioned supine with both the knees and hips flexed 90 degrees. The test is then performed with one hand stabilizing the pelvis and the other hand with the thumb over the hip adductors and the index over the greater trochanter. The hip is slowly abducted, so the dislocated femoral head of slips toward the acetabulum creating reduction (audible and palpable). The positive Ortolani test is a sign of dislocated hip.
Barlow test (provocative test for the dislocatable hip). The child is positioned as for the Ortolani test. The hip is mildly adducted and pressure is applied posteriorly. If the femoral head slips over the posterior rim of the acetabulum and slides back again into the acetabulum when the pressure released, this is considered Barlow positive, which means the hip is dislocatable. Pavlik harness is the treatment of choice of neonates with dislocated hips (positive Ortolani test). In the majority of Barlow-positive neonates, the hips stabilize in the postnatal period. Neonates with a positive Barlow test should have a repeat clinical and hip ultrasound examination after 4 weeks. If the hip is not stable at that time, a Pavlik harness should be used. Surgical treatment is rarely indicated in the postnatal period.
Ortolani test
Barlow test
Pavlik harness
Neonates with short limbs may have a variety of conditions including fibular hemimelia, proximal focal femoral deficiency (PFFD) or tibial hemimelia.
Fibular hemimelia is characterized by congenital complete or partial absence of the fibula. There is no known genetic etiology. The tibia is short with a valgus and procurvatum deformity. There is often a skin dimple at the apex of the deformity and frequently associated with foot deformities. Treatment depends on the foot deformity and degree of limb length discrepancy. The surgical options are limb reconstruction (lengthening and realignment) or amputation of the deformed foot and fitting of prosthesis.
Fibular hemimelia X-ray
Proximal focal femoral deficiency (PFFD)is a congenital anomaly of the proximal femur and pelvis resulting in a short femur and hip deformity. There is no known genetic etiology. The femoral segment is short, abducted, flexed, and externally rotated. There may be genu valgum and anterior cruciate ligament deficiency of the knee joint. The deformity is bilateral in 15% of the cases. Fibular hemimelia may be associated with PFFD and is treated by either reconstruction (limb lengthening and realignment) or amputation.
Proximal focal femoral deficiency
Tibial hemimelia is a congenital partial or complete absence of the tibia. The infant usually presents with a short extremity with a rigid equinovarus, supinated foot deformity.
Preaxial polydactyly is a relatively common associated anomaly. Other congenital anomalies may be associated with tibial hemimelia, such as congenital cardiac anomalies and or spine deformities.
It is one of the few congenital limb deformities that have genetic etiology and is seen with syndromes associated with ectrodactyly (cleft hand and foot deformity). The surgical options are either reconstruction or knee disarticulation.
Tibial hemimelia X-ray
Tibial hemimelia eqinovarus
ectrodactyly
Neonatal foot disorders are relatively common and require careful assessment for proper diagnosis. Examples of the common foot disorders are noted below. Cleft foot is due to an absence of the central two or three rays of the foot. The cone-shaped cleft of the forefoot tapers proximally. Autosomal inheritance is common in bilateral cases and uncommon in unilateral cases. In bilateral cases, the hand may be affected as well (see ectrodactyly, above).
Macrodactyly is an uncommon deformity due to an enlargement of both soft tissue and osseous elements of the toes; it may affect the great toes or lesser toes. The hand and leg may be affected as well. Debulking (excision of bone and soft tissues) procedures are usually indicated.
Foot macrodactly
generalized macrodactly of leg
Polydactyly ischaracterized by duplication of one or more toes. Preaxial polydactyly refers to a duplication of the great toe; postaxial is a duplication of the fifth toe (the most common type—80%). It is less common in central toes. It is more common in African American children. Fifty percent are bilateral, and 30% of patients have a positive family history. There is an autosomal dominant inheritance with variable expressivity. Foot polydactyly is commonly an isolated deformity but may be associated with other syndromes like Ellis-van Creveld syndrome or trisomy 13. Amputation of the extra digit is the treatment of choice.
little toe polydactly
Great toe polydactly
Fibular hemimelia can cause newborn foot disorders with hind foot equilovalgus and missing lateral rays.
Fibular hemimelia foot
Tibial hemimelia can also cause foot deformities in the newborn.
Tibial hemimelia foot disorder
Club foot may be associated with spinal or other anomalies. Usually treated by serial casting.
Club foot anterior view
Club foot posterior view
Vertical talus is an isolated deformity or associated with spina bifida and is bilateral in 50% of cases. Treated with serial casting and selective surgery.
Vertical talus
Calcaneovalgus foot demonstrates equnivalgus of the hindfoot and a normal forefoot. May be associated with posteriomedial bowing of the tibia as shown in the photograph.
Calcaneovalgus foot
Orthopedic injuries or fractures can occur during birth. Clavicular fractures, the most common type of birth fracture, typically occurs during delivery with shoulder dystocia, complete extension of the arm in breech presentations or with large infants.
Clavicle fracture left side
Healing clavicle fracture 3 weeks
Bone Infections. Prematurity, skin infections, and a complicated delivery are known risk factors with hematogenous spread is the most common route of spread. The organisms may gain access to the circulation through venous or umbilical catheters, intravenous feeding lines, or invasive monitoring. The infection usually starts in the metaphysis of long bones. Because the nutrient vessels cross the growth plate to supply the epiphysis, septic thrombophlebitis of these vessels can lead to a growth plate injury and growth disturbances latter in life. The thin cortex and periosteum of the neonate’s bones are poor barriers for infection spread, allowing an infection to be easily spread to the adjacent tissues. When the metaphysis of long tubular bones is intracapsular, these infections usually result in septic arthritis (hip joint, shoulder joints). The osteomyelitis in premature infants or severely ill full-term infants tends to be multifocal with or without septic arthritis (usually two or three sites).
The first radiograph shows septic destruction of both the distal femur and proximal tibial growth plates. The second radiograph demonstrates acute osteomyelitis of the tibia.
Neonatal osteomyelitis 1
Neonatal osteomyelitis 2
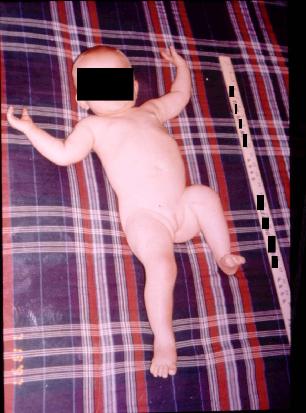
Arthrogryposis multiplex congenitais a syndrome characterized by multiple (at least two or more) joint contractures in multiple body areas (literally the word means “curved joints”). The specific etiology is still unknown. Reduced fetal movement is an etiologic factor. The typical newborn has all the extremities affected. The typical joints contractures are internally rotated shoulders, elbow extension, a pronated forearm, and flexion contractures of the wrist and fingers
Arthrogryposis
Content Copyright McGraw Medical, 2023 New York New York